医療ガスライティングの終焉
医学の忘れられた側面
asyura2.com/24/iryo13/msg/767.html#c4
時々、物事がどれだけ困難であっても、あるいは自分がやっていることにどれだけ疑問を感じ始めても、自分がやっていることは重要であり、続ける必要があることを思い出させてくれる何かに出会うでしょう。
今日、妊娠中の母親と幼い子供を持つ親を対象とした最近の JAMA の調査を見たときに、私にも同じことが起こりました。その調査では、次のような結果が出ています。
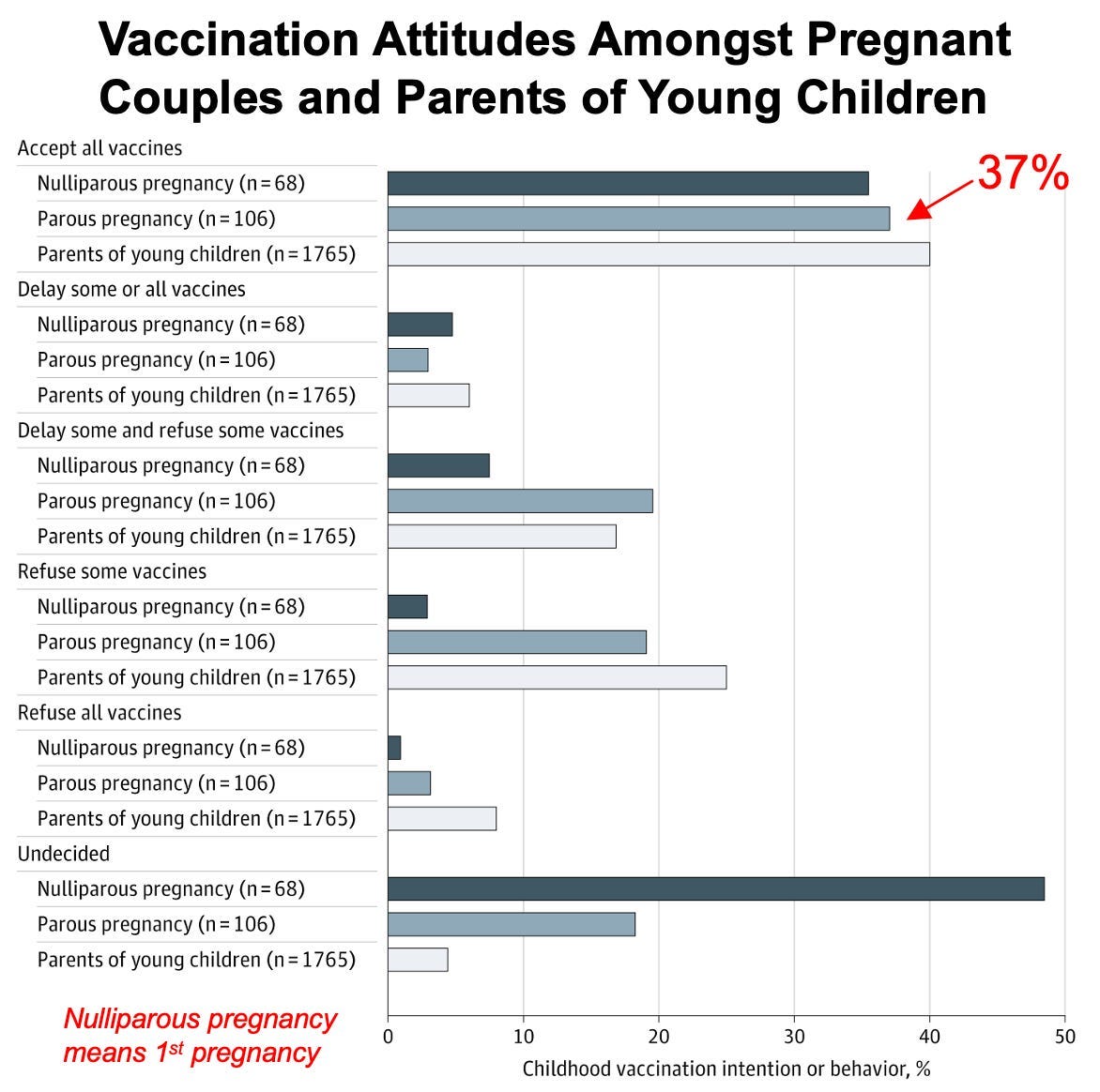
その研究は次のように結論づけています。
出産後の子どものワクチン接種については妊娠中の意思決定に高い不確実性があることを考えると、小児のワクチン接種の決定について家族を積極的にサポートするために妊娠中に介入することには価値があるかもしれない。
COVIDがあまりにも甚大な影響を及ぼしていたため、COVIDカルテルの強欲さがワクチン接種の問題点に人々の目を覚まさせ、既存の小児用ワクチンに対する強い疑念を生むことを期待していました。しかし、これほど大きな変化がこれほど早く起こるとは予想していませんでした。簡単に状況を整理すると、
まず、ワクチン接種に対する信頼は全体的に低下しているものの(これは極めて深刻な問題だと私は考えています)、実際に子供たちにワクチン接種を決断する最年少世代における信頼の低下は、はるかに深刻です。例えば、今年1月に実施された調査の結果を見てみると、全米の37%をはるかに超える人がCDCのスケジュールを完全に信頼し、それに従うつもりだと回答しています。
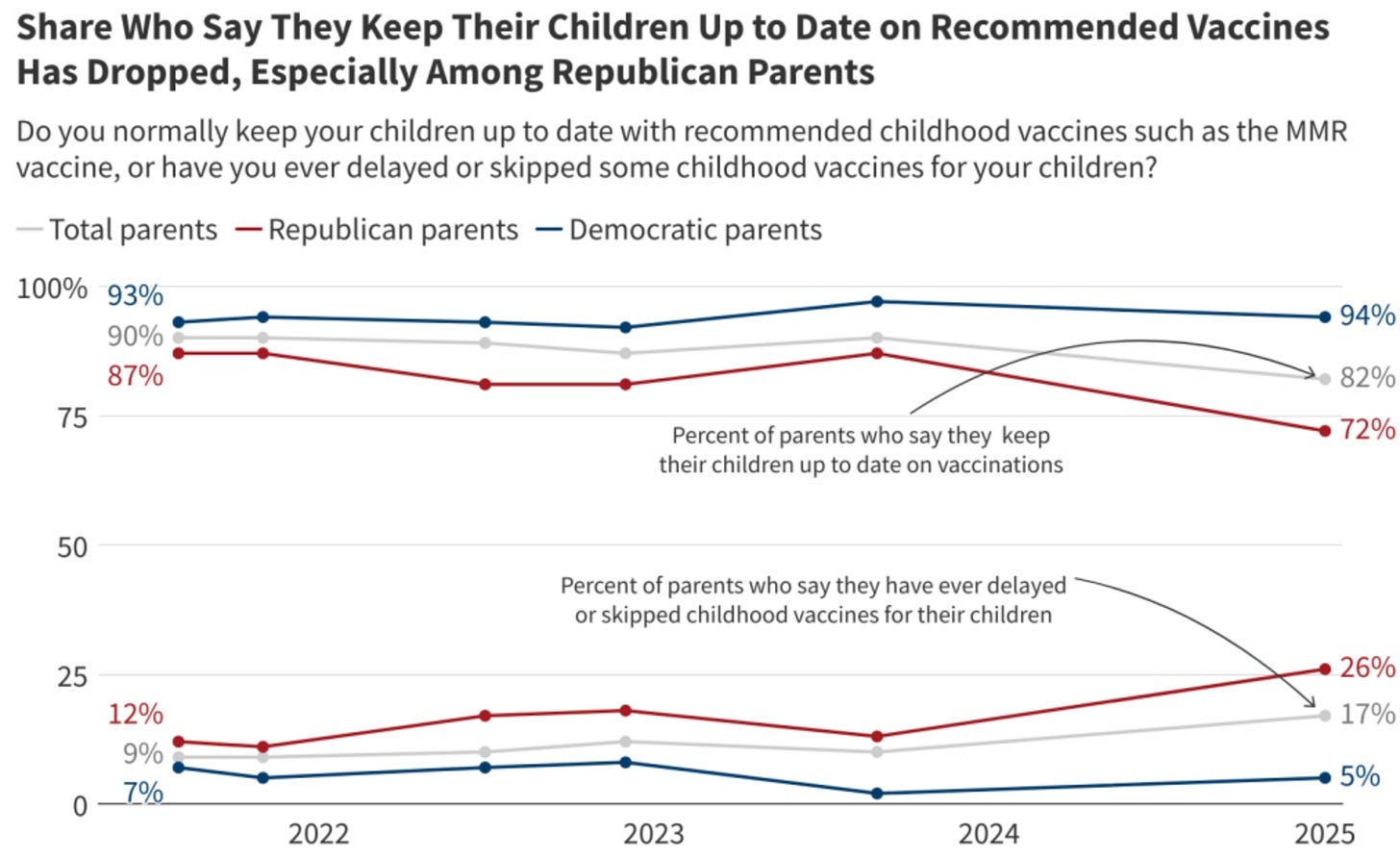
第二に、アメリカの親のうち、スケジュールを完全に信頼しているのは37%です。これは過去の基準値と比較すると大幅に減少しています。具体的には以下のとおりです。
• 2000 年には、 19% の親が「ワクチンに対する懸念」を抱いていました。
• 2003 年には、 28% の親が「ワクチンに対する躊躇」を抱いており、そのうち約 3 分の 2 が特定のワクチンのみを延期または拒否していました。
• 2009 年には、 50% の親が「ワクチンに対する懸念」を抱いており、 11.5% が子供に対する少なくとも 1 つのワクチン接種を拒否していました (最も一般的には、有害な HPV ワクチンの拒否)。
• 2010 年には、小児科医の 89% が、毎月少なくとも 1 つのワクチン接種を親が拒否したと報告しており、毎年の小児インフルエンザの予防接種が最も一般的に拒否されたワクチンでした。
• 2011 年には、 13% の親が代替のワクチン接種スケジュール (一部のワクチンをスキップまたは延期するなど) に従っていましたが、そのほとんどは元々 CDC のスケジュールに従っており、2.2% はすべてのワクチンをスキップしました。
• 2013年には、9%の親がすべての予防接種を拒否または延期し、32%がワクチンの安全性について懸念を抱いていました。
これらの数字を理解する上で重要な背景は、医療現場にとってこれらの数字が警鐘を鳴らすものだったということです。それまでは、ほとんどの親が文句を言わずにワクチン接種を受けるだろうと想定されていました。もし誰かがワクチン接種を遅らせるといった単純な行動で規則を破ろうとすれば(幼少期にワクチン接種を複数回行うと、傷害のリスクが高まるため)、医療現場から非難され、免許を剥奪されることも少なくありませんでした。ですから、彼らが警鐘を鳴らした数字と現在の現実を比較すると、その差はまさに「昼と夜」ほどです。
第三に、ワクチン接種の遵守を強制する主な方法は、社会的圧力(例えば、「みんなが接種しているのだから、接種していない人は頭がおかしいか悪い親だ」など)と義務化です。これらはどちらも、人口の大多数がワクチン接種を受けていることを前提としており、医療業界がワクチン接種率が90%を下回ることを非常に懸念していたのは、まさにこのためです。
そのため、2019年にアメリカ全土で(カリフォルニア州のものなど)、国民の広範な抗議にもかかわらず、非常に多くの不当で強引な幼児期の義務化が推進された主な理由は、ワクチン業界が(非科学的で不当な)ワクチンプログラムを正当化するために必要な大多数の支持を失いつつあることに気づき、そのため、人々にワクチン接種を強制せざるを得なかったためだと
私は考えています。注:2020年に、私は「ロックダウンから私たちを救う」というCOVIDワクチンの非常に積極的なマーケティングキャンペーンが展開されていることに気づきました。そのため、ワクチンキャンペーンは一連のエスカレーション段階を経ると結論付けました(例:ワクチンを奇跡として大々的に宣伝し、その後、希少性を利用して販売する、希少性を解消して引き込まれた他のすべての人を捕まえる、ワクチン接種に対して贈り物をする、公共の場所や企業への訪問に対する社会的制限を通じてソフトな義務化を行う、特定の企業にハードな義務化を導入する、全国的な義務化を行う)。これは、人口の大部分が既にワクチン接種を受けていなければ、後の義務化は実行不可能だったためです(例えば、アメリカの人口の10%がワクチン接種を受けていなければ、レストランは未接種の客を決して出入り禁止にしないでしょう)。そのため、以前は考えられなかった職場での義務化を推進する前に、できるだけ多くの人々にワクチン接種を受けさせることが不可欠でした。それと並行して、カリフォルニア州が特定の学校への義務化(例えば、COVIDワクチン接種)を撤回した数少ない理由の一つは、多くの親が子供を学校から引き離すことを拒否し、喜んで引き離したため、州は結果として得られるはずだった連邦教育予算を失う余裕がなかったことです。
第四に、最近の7月の調査結果を見ると、多くの親が程度の差はあれ「未決定」であることが分かります。これは、ワクチン接種による悲惨な傷害の直接的な事例(特に被害者が親のコミュニティ内に存在する場合)を提供し、ワクチン接種の実際のリスクとベネフィットを明確に示す、信頼できるバランスの取れた情報を継続的に提供できれば、ワクチン接種のパラダイムを永続的に変えることができる真のチャンスがあることを意味します。
私のように多くの人がそうしており、実際に影響を与えていると信じています。さらに重要なのは、RFKジュニアがHHS(保健福祉省)と協力してワクチンによる障害に関するゴールドスタンダードの証拠を公開しようとしていることです。それが公開されれば、ワクチンを拒否する人が多数派になるための基盤が築かれます。これは非常に重要なことです。特に、多くの人が依然としてワクチン接種義務化を主張しているためです(例えば、ハワイの左翼医師知事がまもなく宗教的免除を撤廃し、カリフォルニア州のパン博士のように義務化するだろうという懸念のメールを読者から多数受け取っています。1、2、3)。しかし、アメリカ人の大多数がワクチンを信頼せず、ワクチンを健康と自由に対する不正な攻撃と見なす限り、これらのことはどれも起こりません。
注:これらの傾向は、 443,445人のアメリカ人を対象とした最近のJAMAの大規模な調査でも示されており、2020年4月には71.5%のアメリカ人が医師や病院を信頼していたのに対し、2024年1月には40.1%に減少した。
ワクチンの宣伝
ワクチンに反する実際の証拠はひどいものです(例えば、独立した研究はすべて、ワクチンが様々な慢性疾患を発症する可能性を3~10倍高めることを示しており、深刻な神経学的損傷を引き起こすことを示す文献は1世紀以上にわたり存在します)。そのため、ワクチン市場を維持する唯一の現実的な方法は、ワクチンの安全性に関するすべての独立した研究を禁止し(だからこそ、RFKの政府研究は非常に重要なのです)、国をガスライティングすることなのです。
プロパガンダの本質は、大衆に「売れない」アイデアを売り込むことです。そのためには、論理的ではなく感情的な売り込みが必要です。なぜなら、擁護できないアイデアは議論にさらされるとすぐに消えてしまうからです。そのため、プロパガンダは様々な戦術に依存しており、それらは本質的には感情的なものでありながら、しばしば科学的であると見せかけています。
例えば、プロパガンダの多くは、人々の感情的な反応を引き起こす言葉を使い、メディアがその感情的な反応を集団的に強化することを中心に展開しています。そのため、提示された議論の内容に関わらず、多くの議論は感情的な中傷(例えば、「あなたは人種差別主義者だ」「あなたは気候変動否定論者だ」「あなたは科学を信じていない」「あなたは反ワクチン派だ」「あなたは危険な陰謀の売り込み屋だ」「あなたはインチキ医者だ」)に
堕落してしまうことがよくあります。このため:•非科学的な立場は、しばしばそれを擁護するためのいくつかの偽のスローガンによって構築され、それらのスローガンは、(真剣に議論されるのではなく)対立する議論をかき消すまで叫ばれます。
•望ましい物語をサポートできる、最も感情的に操作的なフレーズ(またはイメージ)を形作るために多くの作業が行われ、その時点でマスメディア全体で大々的に報道され、その後、そのフレーズが自分の考えであると信じ込むようになる一般の人々によって採用されます。
さらに重要なのは、プロパガンダは人々が集団から逸脱することを本能的に躊躇する性質を利用していることです。そのため、どこでも同じメッセージを聞くと(特に仲間もそのメッセージを採用している場合)、ほとんどの人はすぐにそれを採用します。そのため、マスメディアは同じメッセージを集団で繰り返し、そこから逸脱する人々を集団で非難し、現状維持を擁護する「専門家」を次々と登場させ、そして最も重要なことに、反対側の意見を決して聞かないようにしています。
その結果、我が国における医療の主要な問題の多くは、1997年にFDAがテレビでの医薬品広告を合法化する決定を下したことに端を発しています。この時点で、製薬業界はマスメディア最大の広告主となりました。その後まもなく、その経済的影響力はメディアの監視を抑圧するために利用され、製薬業界を問うニュース報道、特にワクチンに関する報道は徐々に排除され、かつて放送されていたような批判的なニュース番組が今日存在することはほぼ想像しがたいものとなっています。
注:シャリル・アトキソン氏のように、この変化を目の当たりにしたニュースキャスターたちは、そのことを証言しています。
真実の独占によって得られた無制限の権限により、ワクチン業界はますます大胆な行動をとるようになった(例えば、より有害なワクチンを市場に投入し、より厳格な検閲を実施し、そしてより厳格な規制を実施するなど)。幸いなことに、突如権力を握った多くの人々と同様に、彼らは度を越し、大きな反発を引き起こし、業界を史上最悪の状況に陥れたと言えるだろう。
これは、傷害の増加(子供が受けるワクチンが増えるほど、傷害も増える)に加えて、マスメディア全般に対するさらに大きな反発が起こり、ワクチン接種のような人気のない報道をマスメディアが制御し続けることがはるかに困難になったためです。
注:ここ数十年、特にここ10年ほど、メディアは(どんなに無意味であろうと)自らの主張を強引に主張し、反対意見を全て抑圧するようになりました。インターネットが社会構造に深く根ざし、良質なコンテンツ(例えば、大衆が反発するマスメディアの嘘を暴くコンテンツなど)が瞬く間に拡散するようになったため、既存のモデルはもはや機能しなくなっています。むしろ、既存のモデルが強化されればされるほど、人々は信頼を失っていくのです。
医療上の傷害を歪める
私の病的な趣味の一つは、医薬品がどのように人を傷つけ、障害を負わせるかを研究することですが、その中でも、身体的な問題だけでなく精神的な問題も引き起こすものは特に残酷だと思います。
例えば、SSRI系抗うつ薬には多くの一般的な副作用(例:性機能障害、双極性障害、感情麻痺、ひどい離脱症状、そして時には精神病的な暴力)があり、その多くは患者に「正気を失う」ような感覚を引き起こし、薬の服用を中止したいという強い欲求を引き起こします。しかし、医師は薬が患者を傷つけていることを認識せず、これらの副作用は薬の一般的な副作用ではなく、患者自身の精神疾患によるものだと伝えることがよくあります。
そのため、患者は薬を飲み続けるように言われることになります。さらに、「精神疾患」の患者はしばしば自己判断能力が欠如しているとみなされるのに対し、精神科医は権威者とみなされるため、誰もが(例えば、患者の家族や(しばしば治療を義務付ける)裁判所など)患者ではなく精神科医の味方をし、副作用は患者の精神疾患によるものだと主張し、患者
にさらに多くの精神科薬を服用させるというケースを、私は数え切れないほど見てきました。注意:薬の副作用で現実感覚を失い、自分の判断に疑問を抱き始める患者、あるいは諦めて周囲の権威者を盲目的に信じるべきか、といった状況になると、この状況はさらに困難になります。
精神医学が患者をガスライティングする典型的な方法には次のようなものがあります。
•現れた症状はすべて既存の精神疾患によるものだと伝える。
•患者が薬の副作用を経験した場合、副作用を認めるのではなく、投与量を増やす。注:これは悲惨な学校銃乱射事件の
直前によく見られる話ですが、精神医学の分野ではSSRIが患者を精神病にする可能性を広く否定しているため、残念ながら、このことが認識されることはほとんどありません(そのため、何度も同じことが起こるのです)。
•患者が離脱反応を経験した場合(これは非常に一般的であり、SSRIの最も陰険な問題の一つです)、その副作用は患者が(精神疾患を治療していたので)薬を「必要」としていたことを証明するものだと患者に伝え、危険な離脱症状として認識させるのではなく。
•患者が新たな精神症状(例えば躁病)を発症した場合、薬が症状の「原因」ではなく、以前から存在していた精神疾患が薬によって「顕在化した」と説明されます(患者がそもそも薬を使用していなければ、その症状が「顕在化」することは決してなかったはずですが)。例えば、双極性障害はSSRI長期服用者の約25%が発症する衰弱性疾患です(そのため、SSRIの大量投与が始まって以来、双極性障害の蔓延につながっています)。そして、この疾患があまりにも一般的であるため、「顕在化した」という話は、多くの精神科医が患者に及ぼされる害を正当化するために用いる常套句となっています。
悲しいことに、ガスライティングは精神医学に限ったことではありません。例えば、市販されている毒性の高い薬の臨床試験の多くで、治験参加者は深刻な副作用を発現しましたが、製薬会社の承認を確実にするために、臨床試験の調査員はそれらの反応を治験参加者と政府の両方から隠蔽しました。例えば、私は以下においてこれがどれほどひどいことが行われていたかを詳しく述べました。
• SSRIの臨床試験。
• HPVワクチンの治験。
• COVIDワクチンの治験。
注:COVIDワクチンの治験で起こったことについて内部告発者が共有したことに多くの人が愕然としました(例えば、誰もが彼らに受けた明らかな傷害が「本当」ではなかったと言ったなど)。しかし、私がそれらの記事で説明しようとしたように、これらは実際には治験における長年の課題です(治験の実施には多額の費用がかかるため、製薬スポンサーは治験で薬が「安全で効果的」であることが示されたことを「証明」するためにあらゆる手段を講じます)。
医師は、「公平な」臨床試験で傷害の存在が証明された場合のみ、傷害が「現実」である(逸話的な偶然や患者の頭の中で単に想像したのではなく)と信じるように訓練されているため、臨床試験で見られるガスライティングは、世界中の医師が臨床試験で示されたことが真実であると信じ、臨床試験で隠蔽された(そのため最終的な臨床試験報告書には記載されなかった)自分の患者の同じ傷害を無視することになるため、ガスライティングの連鎖を引き起こします。
注: 多くの異なる薬物が、精神障害と誤診される神経損傷 (特に感受性の高い人々) を引き起こすため、これは大きな問題を引き起こします。特に、それらの患者はしばしば精神漏斗に送り込まれ、その時点でさらに神経を破壊する薬物を投与されるからです。
ガスライティングとは何ですか?
虐待者が被害者を支配する典型的な方法の 1 つは、環境を操作して、虐待を受けた個人が目の前で何が起こっているかに関係なく、自分の観察を疑い始めるようにすることです。
1944年の映画『ガス燈』では、悪役の夫(シャルル・ボワイエ)がガス灯の吸気口を調整してちらつかせると同時に、精神的に虐待を受けている妻(イングリッド・バーグマン)に何の変化も起こっていないと主張しました。ガスライティングという言葉は、この名作映画に由来しています。
現代では、医療提供者(そして多くの場合マスメディア)が、患者の傷害は医薬品(または問題となっている他の医療処置)とは何の関係もないという同じメッセージを繰り返すことによってこれが達成され、患者自身の精神疾患のせいにされることが多々あります。
話を進める前に、負傷した患者として、これがどれほど悲惨な経験であるかを強調しておきたいと思います。もし(医療上の負傷により)これまで知っていた世界が崩壊し、信頼していたすべての人(「専門家」の判断を重んじる友人や家族も含む)から「これはすべてあなたの気のせいで、精神科の助けが必要だ」と言われたらどうなるか想像してみてください。まさに正気を失うための完璧な処方箋です。
例えば、青少年層におけるCOVID-19ワクチンの安全性を主張するために使用された、ファイザー社の重要な試験におけるマディ・デ・ガレイの経験を考えてみます。

マディさんの体験は悲惨なものでしたが、悲しいことに、他に類を見ない出来事ではありませんでした。COVID -19ワクチンの治験では、他にも多くの人が同様の経験をしました。同様に、医療制度によって被害を受けた他の人々からも、同様の話をたくさん聞いてきました。ほとんどの医薬品には、特定の患者に悪影響を及ぼす程度の毒性があるからです。
西洋医学(アロパシー)の実践には、常にこの毒性がつきまとうため、医療従事者は、避けられない医療上の損害が業務に支障をきたさないようにするための戦略を徐々に確立してきました。これは基本的に、以下の方法で達成されてきました。
•患者に、経験した有害事象は実際には発生していないか、毒性のある医薬品とは無関係であると伝える。
•これらの傷害と市販の医薬品との関連を否定する証拠を提供する精巧な科学的装置を開発し、同時に国民が自らの観察を信頼するのではなく、科学的コンセンサスに従うように訓練する。
• 同様の程度の固有の毒性がない競合する薬剤を違法にし、既存の医療市場における唯一の選択肢を毒性のある薬剤にします(同様に、現代医学は常に最良の薬剤と考えられており、他のすべてのアプローチはそれに追いつく方法を見つけなければならないことを考えてみてください)。
これは、あらゆる治療にはリスクがあり、その治療はリスクを上回るメリットがあるため選択される(リスクのない医療システムを単に検討するのではなく)という医学の原則がここにある理由でもあります。
これらすべてが、医療ガスライティング、あるいは「対症療法があなたをガスライティングで死に至らしめる」と言われる悲劇的な現象を引き起こします。
医師はなぜ医療上の傷害を診断できないのか?
私は 1700 年代後半まで遡る医療ガスライティングの記録された例を数多く見つけましたが、それぞれのケースで、発生している傷害が医薬品に関連している可能性があることを認めようとしたのは、医療従事者のごく一部だけでした。
同時に、私が邪悪だと思うような医師に出会うことは稀です。それどころか、ほとんどの医師は驚くほど知的で善意にあふれ、患者のために心から最善を願う人々です。
現時点では、医療ガスライティングは私たちの訓練の自然な帰結であると考えています。対症療法の治療ツールは非常に限られているため、ほとんどの医師は患者に安全でない医薬品を投与せずに診療を行うことはできません。そのため、自己同一性を保つために、彼らは自分の医薬品を完全に信じ込まざるを得ないのです(詳細はこちらで詳しく説明しています)。
医師になるということは、個人として多大な投資を要し、その過程を経た人にとって、自分が学んだことの多くが非常に疑わしいものであることを認めるのは極めて困難です。
同様に、善意の医師は患者に危害を加えたいとは思っていません。そして、実際に危害を加えることがよくあるため、反射的な心理的対処メカニズムとして、発生するあらゆる傷害の可能性を否定することになります。
私がこのことに初めて気づいたのは、ある医師が講義の中で反ワクチン派への激しい非難を挟み込み、「…考えてみてください。小児科医がワクチンが患者に危害を加える可能性があると考えている場合、本当にワクチンを接種すると思いますか?」と締めくくった時でした。
対症療法(アロパシー)がもたらす害悪が広く否定されていることが、私の専門分野がガスライティングに傾倒する一因となっている可能性はありますが、それが根本的な問題だとは考えていません。むしろ、医師が受ける訓練によって医学的損傷を認識できなくなっている結果であると考えています。
医学的失明の起源
人体は非常に複雑なため、どの時代においても、人間は体内で起こっているあらゆる事象を把握することが非常に困難です。ほとんどの医療システムは、この課題に対処するため、各患者に内在する膨大な複雑さを、患者の健康にプラスの影響を与えるために焦点を当てるべき重要な点にまで単純化する診断モデルを構築しています。
このアプローチの欠点は、各患者において、評価に用いられる診断モデルの枠に収まらない要素が常に存在することです。そうなると、当然のことながら、医師が非常に有能で偏見のない観察者でない限り、それらの要素を認識することはできません。
標準的な医学では、多くの事柄(特に医薬品の処方の適応)を特定するのに優れた診断モデルが教えられています。しかし、そのモデルは健康とウェルネスにとって非常に重要な他の多くの要因を考慮できていません。
例えば、医学の多くは、線形アルゴリズムに組み込んだ一連のリストを暗記するという方法で教えられます。これは多くの複雑な主題を「はい」か「いいえ」の二項対立に分解する必要があるため、この二項対立の間にある多くの重要なことが、翻訳によって失われてしまいます。
これは神経系で説明するのが最も簡単です(ただし、この問題は神経系に限ったものではありません)。評価する際に、私たち全員が教えられていることの一つは、12個の脳神経が正常に機能しているかどうかを素早く確認することです(例えば、飲み込むことができるか、笑うことができるか、指の動きを目で追えるかなど)。
多くの場合、頭蓋神経は「概ね正常」であっても、発火に何らかの問題を抱えています(例えば、眼球が左右に動く際の運動弧のどこかの時点で、スムーズに動くのではなく、飛び跳ねるなど)。こうした「軽微な」障害(ワクチンによる傷害による微小脳卒中によく伴う)は、患者の生活の質に重大な影響を与えることが多いのですが、ほとんどの場合(経験豊富な神経内科医や脳神経外科医による評価を除く)、これらの神経の機能は正常とみなされ、無視されます。そのため、周囲で多数のワクチンによる傷害を目にする医師は、同僚から疎外され、解雇されてしまうのです。
病気をシンプルにする
残念ながら、脳神経の例は、複雑な症状が単純化されて一つの箱に押し込められ、都合の悪い診断が認識されないままにされる多くの事例の一つに過ぎません。このような箱詰めが行われるもう一つのよくある例は、複雑な現象が実際には何であるかを明言することなく、権威ある診断を用いてそれを否定することです。
例えば、医学における多くの疾患は、ラテン語で書かれた単なる症状です。皮膚炎は文字通り「皮膚の炎症」と訳されますが、ほとんどの場合、炎症の原因を解明しようとするのではなく、炎症を抑えるクリームで治療するだけです。
逆に、他の多くの医療システムでは、皮膚の炎症は体内の異常を示す重要な兆候と認識されており、炎症の正確な性質と発生部位を綿密に検査することで、炎症の根本原因を特定し、対処しています。
注:皮膚科ではある程度この認識が認められていますが、皮膚科でも、本来あるべき程度には認められていません。
その結果、患者が抱える一般的な病気の多くは、一つ、あるいは数個の共通の原因を抱えていることがわかりました。しかし、ほとんどの場合、たとえその分野のトップクラスの専門医が診察したとしても、根本的な病理は治療過程を通して十分に検査も理解もされていません。こうした状況は、医療制度が、個々の患者の病状の固有の状況を理解しようとする努力を奨励するように構築されていないことが原因だと私は考えています(医師は患者の症状を標的とした治療薬を処方するのに数分しか割かず、最終的に効果が現れることを期待しているのです。これは同時に、これらの医薬品の害がしばしば無視されていることを意味します)。
医原性に関する議論の枠組み
医原性(いんげんせい)とは、医療行為への不適切な反応(例えば、手術や薬剤による合併症など)に起因するあらゆる種類の病気や医学的合併症を指す用語です。私が数十年にわたって観察してきたよくあるパターンは、誰もが特定の医原性合併症の存在を否定し(例えば、「証拠がない」など)、その後、その存在を示す圧倒的な証拠が現れると、その合併症が認められるというものです。
これが起こると、薬物による害は、受け入れられた害だけが悪いと捉え直され、他には合併症の可能性はないという根底にある仮定が作られます。
たとえば、フルオロキノロン(シプロなど)は、人体に重大な害を及ぼす可能性のあるかなり毒性の強い抗生物質であり、その毒性と潜在的な利点が釣り合わない多くの軽度の感染症(尿路感染症など)に頻繁に投与されます。
医学部では、腱断裂(独特で無視しがたいもの)がこれらの薬の副作用であると誰もが学びます。その結果、医師が害を評価するとき、腱断裂を探すことになりますが、フルオロキノロンによる他の十分に文書化された合併症のほとんどを認識することはできません。
最近、J&J社のCOVID-19ワクチンでこの再構築が見られるようになりました。「ワープ・スピード作戦」の開始当初、私はmRNA技術を市場に投入することが主要な目標だと仮説を立てました。なぜなら、mRNA技術は製薬業界に将来的に数兆ドルの収益をもたらす可能性を秘めていたからです(しかし、安全性に課題があったため、「緊急事態」でもない限り、ヒトへの臨床試験への障壁を打ち破ることはできないでしょう)。
そのため、ワクチンの安全性に関する懸念が浮上すれば、mRNA技術を「安全」に見せるために、非mRNAのCOVID-19ワクチンが犠牲になるのではないかと私は疑っていました。そして、まさにJ&Jワクチンの接種でそれが起こりました。極めて異例な血栓症が6件報告され、FDAとCDCは11日間ワクチンの接種を一時停止しました。
そうすることで、FDA はワクチンの副作用を綿密に監視しており、ごく少数の人々にまれな副作用が発生した場合にはワクチンを撤回する用意があるという認識が生まれた。
mRNAワクチンはJ&Jワクチンよりもはるかに多くの血栓を引き起こしており、これは真実からかけ離れた話です。同様に、FDAはCOVID-19ワクチンに関する際限のない警告を無視しているという調査が相次いでいます。
残念ながら、この策略は(一時的に)成功し、1年以上もの間、ワクチンの安全性について議論する医師の話をたまに聞くと、彼らが最もよく使う議論の1つは、FDAが血栓が6回発生した後にJ&Jのワクチンを一時的に停止するのであれば、mRNAワクチンにもっと大きな未解決の問題があるはずがない、というものだ。
同様に、CDCはCOVIDワクチンに重大な副作用はないと主張し続けてきましたが、最終的には心筋炎を引き起こす可能性があることを認めざるを得ませんでした。その時点で、心筋炎は非常に軽微である(これは事実ではありません)と述べ、COVID-19はワクチンよりも心筋炎を引き起こす可能性が高い(つまり、全体としてワクチンは実際には心筋炎を予防する)と方向転換しましたが、これもまた事実ではありません。そのため、ワクチンの副作用を「唯一の問題は、時折短時間の心筋炎を引き起こすことだが、それは非常に軽微であり、実際の心筋炎の問題はCOVID-19によるものであることは明らかである」と言い換えようとする試みが数多くなされてきました。
精神疾患合併症および医原性傷害
上記の点が示すように、医師が医療傷害の存在を認識する上で、様々な要因が阻害要因となります。そこで問題となるのは、避けられない傷害をどのように説明するかということです。
ご想像のとおり、デフォルトの戦略は、傷害を漠然とした診断名に包み込み、その診断名が医学的傷害の責任を負い、傷害を受けたすべての人にそのレッテルを貼ることです。これは通常、精神医学的診断で行われますが、最近ではCOVID-19感染症もその役割を担っています(これらの診断名はどちらも、ワクチンの臨床試験で患者をガスライティングするために使用されました)。
私が見つけたこのガスライティングに関する最も古い言及は、フロイトの時代に遡ります。フロイトは新しい精神分析モデルを用いて、医師が理解に苦しむ患者の複雑な症状を説明しました。しかし、『自閉症の時代:水銀、医療、そして人為的な疫病』で詳述されているように、フロイトの症例研究に対する外部からの評価は、これらの患者の多くの問題が実際には水銀中毒に起因することを示唆しています。
水銀は極めて毒性が強いにもかかわらず、何世紀にもわたって医療現場で使用されてきました(そして、ある程度は今でも使用されています)。水銀中毒の患者は、神経学的および精神医学的合併症(他の多くの病状と同様に、「女性ヒステリー」とされることが多かった)を含む、多岐にわたる複雑な疾患を発症することがよくありました。
これらの合併症は医師ではなく患者の責任(例えば、未解決の性欲の結果)であるというフロイトのメッセージは、医療界にとって非常に魅力的なメッセージであり、結果として党の方針となった。
それ以来、神経損傷が精神症状を引き起こす可能性があることが体系的に認識されておらず、むしろ神経症状は、心理カウンセリングと精神科薬物療法による治療を必要とする、既存の精神疾患の兆候とみなされています。
この問題の最も良い例の 1 つは「機能性神経障害 (FND)」です。これは、脳に何らかの異常があることが認識されますが、説明が見つからないため、既存の精神疾患によるものと推定されます。
国立衛生研究所のFND に関する説明を再確認すると、上記の説明が誇張ではないことがわかります。FND はワクチンによって障害を受けた患者が受ける最も一般的な診断の 1 つであるため、ワクチンによって障害を受けた患者が経験していることを聞くと非常に悲しいことです。
FND の症例 (例えば、発作を特徴とする症例) を見ると、障害の原因は頻繁に見つかりますが、神経科医 (私の友人も含む) は実際の原因を考慮したくないため、診断に必要な検査は患者を担当する医師に指示されなかったり、医師によって知らされなかったりすることがよくあります。
マディの話を振り返ってみると、まさにこれが彼女に起こったことであり、ワクチン接種による彼女の永久的な麻痺は、精神疾患に起因するFNDと診断されたことに気づくでしょう。このガスライティングのせいで、彼女はワクチンに対する神経学的反応が起こった際に適切な治療を受けることができませんでした(適切な治療を受けていれば、おそらく永久的な障害は防げたはずです)。
これは、主任研究者が、参加者1人に重度の神経学的反応が出ればワクチンが子供にとって危険すぎることを十分に認識していたため、マディの怪我が治験に影響しないようにガスライティングをしようとしたためだと私は考えています。さらに悲しいことに、マディの経験は珍しいことではなく、治験参加者から得た証言は、COVIDワクチンの治験において組織的な不正があったことを明らかに示しています。
医師が医療事故の原因として挙げるもう一つの一般的な症状は「不安」です。このプロセスには2つの大きな問題があります。
人生を変えるような怪我をすると通常は苦痛が生じることを認識していないこと、そして同様に、医療従事者による集団的なガスライティングを受けることが誰の精神衛生にも良くないことを認識していないこと。さらに悪いことに、医薬品による傷害はしばしば組織損傷を引き起こし、それが不安を誘発します。
注:さらに、多くのマスメディアは、現在の製品や物語を売り込むために、将来への不安を煽ることで私たちをコントロールしています。
残念なことに、神経系への損傷(医薬品の一般的な毒性)が精神疾患を引き起こす可能性があることを認識している医師はごくわずかです。彼らは、精神的苦痛が神経症状を悪化させることが多いことを認識しているだけで、精神的苦痛が神経疾患の根本的な原因となることははるかに稀であることを認識していません。
同様に、多くの一般的な精神疾患には器質的な原因(例:診断未確定の慢性感染症、外傷性脳損傷、栄養失調や代謝不全)があります。しかし、多くの場合、精神科医は根本的な原因を調べるのではなく、患者の症状(例:うつ病なのでプロザックが必要)に基づいて薬を処方します。
これは、前者を行うと報酬が高いが、後者は通常は報酬が高くなく、精神科医の研修でも重視されないためだと私は考えています。
神経損傷は精神疾患(例えば、迷走神経機能不全による不安など)を引き起こすことがよくあるだけでなく、他の臓器系への損傷も同様に精神疾患を引き起こす可能性があります(漢方医学はこれらの相関関係を非常にうまく解明しています)。COVID-19ワクチンに関して私が目にした最も顕著な例の一つは心臓に関するもので、2021年以降、以下のような会話を何度も重ねてきました。
友人:ワクチン接種を受けてから、ひどい不安発作に悩まされています。心臓が激しく鼓動し、胸が痛くなるんです。以前はこんなことはなかったのですが、今は何もかもが不安で、落ち着くのがとても難しいんです。
私:心臓を診てもらった方がいいよ。
友人:どういう意味?みんなストレスによる不安症だと言ってたよ。
私:信じてよ、心臓を診てもらった方がいいよ。
(時間が経つ)
友人:どうして心筋炎だって分かったの?
心臓(または迷走神経)の損傷は、しばしば不整脈や胸痛を引き起こし、動悸はしばしば不安を誘発します。残念ながら、これらの症状も不安によって引き起こされるため、医師はこれらの症状が見られると、不安症と診断し、それ以上の診察は行わないことがよくあります。
注:このガスライティングは非常に一般的で問題視されていますが、精神科患者の中には妄想(または不誠実)に陥り、実際には存在しないものを見ている患者もいることを認識することが重要です。そのため、実際に医学的な傷害を抱えた困難な患者も、しばしばそうした患者と同じカテゴリーに分類され、善意の医師であっても、このことを認識していても、自分の患者にどのシナリオが当てはまるのか完全には判断できない状況に遭遇することがあります。
医療パターナリズム
基本的に、次の 2 つの医療実践モデルが採用されています。
父権主義的なモデル(医師の言うことすべてを疑うことなく信じて従うことが期待されるモデル)。
医師があなたの健康のために協力する協力モデル。
西洋医学の歴史の大部分において、父権主義的なモデルが標準となっていましたが、近年では協働的なモデルが推進されています。現在、多くの患者が協働的な医師を求めています(特に、システム医師はチェックリストの確認に多くの時間を費やす必要があり、患者と実際に関わる時間がほとんどないためです)。そして、市場はこうした変化に取り組む医師に経済的に報いています。
医師に関して多くの人が抱いている大きな誤解の一つは、医師は絶対に間違いを犯さない存在だということです(これは父権主義的なモデルを正当化する大きな根拠となっています)。しかし実際には、白衣の裏側を覗き込むと、私たちも皆さんと同じような多くの問題を抱えています。このことを真に認識し、診察を受ける医師を同じ人間として敬意を持って扱うことは、協力的な医師と患者の関係を築くための最も効果的な戦略の一つです。
医師が、被害者に対して自己中心的な理由でガスライティングを行うこともあります(例えば、ファイザー社のワクチンの臨床試験での使用を守るため、あるいは訴訟から医師を守るという極めて誤った考えからなど)。しかし、ほとんどのケースは、医師が実際に被害に遭ったことを認識していないことが原因だと私は考えています。その結果、これらの医師は患者のために最善を尽くしていると信じていますが、実際にはガスライティングを行っているに過ぎません。
現代社会における最大の問題の一つは、私たちが自分自身や他者からどれほど疎遠になっているかということです。医師と患者の関係において、この疎遠さは、医師が患者に何が起こっているのか(例えば、医療上の怪我など)を認識すること、あるいは他の医療従事者が患者をガスライティングしている中で、患者のために闘わなければならないと感じることを困難にしています。
ガスライティングを避けるための最善の選択肢について尋ねられたとき、私は以下の選択肢のいずれかを追求することを提案します。
1) 保険診療ではなく、直接料金を支払う医師に診てもらう。このビジネスモデルは、医師が患者と医師の協力関係を築き、ビジネスを維持していくことを強いるため重要です(ガスライティングを受けただけでは、誰も料金を支払ってはくれません)。私は「支払った分だけ得られる」という言葉を強く信じており、保険診療を基本とするシステム医師にしか診てもらえないと、良い結果が得られないことが多いです。
例えば、この記事の草稿を書き上げる少し前に、ある患者さんが診察を受けました。その患者さんは、 25年間にわたって人生に大きな影響を与えてきた、比較的単純な問題を抱えているように思えました。病歴を調べてみると、この患者さんは12人もの(保険診療の)医師にかかったそうです。その多くは、専門分野の高度な処置で問題を解決できると約束していましたが、結局、何の効果もなかったか、症状を悪化させるだけでした。
彼の話で印象的だったのは、問題の原因を解明するために徹底的な評価を行ったことのある人が 1 人しかいなかったことです。
2) 自費診療の医師を受診することは多くの場合素晴らしい投資となるものの、多くの患者は経済的に余裕がありません。このような場合、理想的なシナリオは、口コミで保険診療を受け付けている医師を見つけ、医師と患者の協力的な関係を築くことで評判を得ていることです。残念ながら、このような医師を見つけるのは難しく、また、これらの医師は往々にして診療内容が充実しており、なかなか診察を受けることができません。
3) 3 番目 (多くの場合、唯一の選択肢) は、医師を「医師」としてではなく、同じ人間として扱い、敬意を持った態度で医師との協力関係を自ら築くことです。
一般的に、このアプローチは、最近医療研修を終えたばかりの医師(年齢を重ねるにつれて誰もがより厳格になり、初期の段階では診療所がまだ満員ではない)や、医師の診察時間が長くなる医療現場(10~15 分で協力関係を築くことは実際には不可能)で最も効果的です。
どちらの選択肢を選ぶにせよ、医療傷害の発生を裏付ける文書を提出することがしばしば重要です。これには、医療処置後の傷害の経過を示す記録や、両者の関連性を裏付ける科学文献などが含まれます。
一方、医師(特に若い医師)は、この関連性について、対立的な態度ではなく、落ち着いて思慮深い方法で提示されれば、最も受け入れやすいでしょう。なぜなら、他の人間と同じように、彼らも防御的になりがちだからです。ガスライティングを受ける過程がどれほど心を痛めるかを考えると、この態度を維持することは非常に困難です。
しかし残念なことに、それは必要なことです。なぜなら、医師は薬害を心理的な性質のものとして見るよう訓練されており、患者がその状況について完全に正当な感情を表明すると、患者の精神的健康に関する医師の誤った認識につながることがよくあるからです。
結論
政府が衰退するたびに、その嘘の大胆さはますます増していきます。これは、私たちもメディアを通して(ワクチンに関しても、政治プロセス全体に関しても)目にしているものです。このアプローチは非常に効果的ではありますが(どれほど多くの人がいまだにこの物語を信じているかを考えてみてください)、同時に、ある程度の段階を過ぎると、誰もが目覚め始めます。特に、嘘を文脈の中で捉える枠組みがあればなおさらです。
言い換えれば、今私たちが目にしている社会変化の多くは、目の前で起こっている出来事について、マスメディアが過剰なガスライティングを行うことに人々がうんざりしているからこそ生じているのです。メディアには、この問題に対処する選択肢が二つしかありません(さらなるガスライティングか、真実を伝えるか)。しかし、真実を伝えても権力(あるいは金)を手放すことはできず、ガスライティングを繰り返すことで、社会からの信頼を低下させる悪循環に陥っているのです。
医療ガスライティングは、私が医療において最も嫌悪するものの一つであり、この出版物の主な目的の一つは、この概念に注目を集めることです。そのため、COVID-19の影響(そして患者と医師の両方がワクチンによる障害について受けた深刻なガスライティング)により、特にCOVID-19ワクチンによる医原性障害の可能性に対する受容性がはるかに高まっていることを目の当たりにし、非常に勇気づけられました。今起こっていることは、私がこれまで見てきたものとは全く異なります。それは主に、医療ガスライティングがついに終焉に向かうかもしれないことに、皆さん一人一人、そして私自身深く感謝しているからです。特に、医療産業複合体は今、信頼の喪失により多額の損失を被っており、失われたビジネスを取り戻すために真実を語り始めざるを得ない経済的状況に追い込まれています。
この出版物とそれが生み出したコミュニティから他の読者がどのように恩恵を受けているかを知るには、こちらからフィードバックをご覧いただけます。また、「Forgotten Side of Medicine」に掲載されたすべての記事の索引は、こちらからご覧いただけます。
この投稿に関する議論



Ending Medical Gaslighting
How the institution of medicine covers up the inevitable harms of its unsafe therapeutic toolbox.
Every now and then, regardless of how difficult things are or how much you begin to doubt what you are doing, you will come across something that reminds you that what you are doing matters and you need to continue.
That happened to me today when I saw a recent JAMA study surveying pregnant mothers and parents of young children, which found:
That study, in turn, concluded with:
Given the high decisional uncertainty during pregnancy about vaccinating children after birth, there may be value in intervening during pregnancy to proactively support families with childhood vaccination decisions.
As COVID had been such a severe overreach, I had hoped that the COVID cartel’s greed would awaken people to the issues with vaccination and prompt significant skepticism against the existing pediatric vaccines. However, I did not expect such a large shift to occur so quickly. To briefly put this in context:
First, while there has been an overall loss of trust in vaccination (which I consider to be absolutely profound), the drop in confidence is much greater among the youngest generation, who are actually making the decisions to vaccinate their children. Consider for example, the results of this January survey, where far more than 37% of all Americans fully trusted and intended to follow the CDC schedule.
Second, a total of 37% of American parents fully trust the schedule, which represents a massive drop compared to the historical baseline. Specifically:
•In 2000, 19% of parents had “concerns about vaccines”
•In 2003, 28% of parents had “vaccine hesitancy,” of whom approximately two-thirds delayed or refused only certain vaccines.
•In 2009, 50% of parents had “concerns about vaccines” and 11.5% had refused at least one vaccine for their child (most commonly refusing the injurious HPV vaccine)
•In 2010, 89% of pediatricians reported at least one vaccine refusal by a parent each month, with yearly childhood flu shots being the most commonly refused vaccine.
•In 2011, 13% of parents followed an alternative vaccine schedule (e.g., skipping or delaying some vaccines)—most of whom had originally followed the CDC schedule, along with 2.2% skipped all vaccines.
•In 2013, 9% of parents declined or postponed all immunizations, and 32% had concerns about vaccine safety.
The key context to understand about these figures is that they were alarming to the medical field, as their baseline had been to expect almost all parents would vaccinate without complaining and if someone dared to step out of line by doing something as simple as delaying vaccines (as more vaccines close together at a young age increases the likelihood of an injury) they were crucified by the medical field and often lost their licenses. As such, if you consider the figures they were alarmed by, and then compare them to the current reality, the difference is essentially “night and day.”
Third, a major way vaccine compliance is enforced is through social pressure (e.g., “everyone else is doing it, so you must be crazy or a bad parent if you aren’t”) and mandates. Both of these are predicated on the majority of the population being vaccinated, which essentially is why the medical industry was so concerned about vaccine use dropping below 90%.
As such, I believe a key reason why so many unconscionable and aggressive childhood mandates were pushed across America in 2019 (e.g., the California ones), despite widespread public protest, was because the vaccine industry realized they were losing the majority necessary to justify (an unscientific and unconscionable) vaccine program and hence had to default to forcing them to vaccinate.
Note: in 2020, I realized a very aggressive marketing campaign was being made for the COVID vaccines which would “save us from the lockdowns.” Because of that, I concluded that the vaccine campaign would go through a series of escalating stages (e.g., mass promoting the vaccine as a miracle then selling it on scarcity, remove the scarcity to catch everyone else who’d been pulled in, give gifts for vaccinating, create soft mandates through social restrictions on visiting public areas or businesses, introduce hard mandates at certain companies, create nationwide mandates). This was because the later mandates were unviable unless most of the population was already vaccinated (e.g., if 10% of America was vaccinated, restaurants would never ban unvaccinated customers), so it was critical to vaccinate as many people as possible before trying to push the previously inconceivable workplace mandates. In parallel, one of the only things which has ever gotten California to back down on certain school mandates (e.g., for the COVID vaccines) was so many parents refusing and being willing to pull their kids out of the schools that the state could not afford to lose the Federal Education dollars that would have resulted in.
Fourth, if you look at the recent July results, you will notice that many parents are, to varying degrees, “undecided.” What this means is that we have a real chance to permanently change the vaccine paradigm if we can provide both direct stories of tragic vaccine injuries (especially if the injured party is within the parent’s community) and if we can continue to provide trustworthy and balanced information that clearly shows the actual risks and benefits of vaccinations.
Many like me are doing that, and I believe we are having a real impact. More importantly, RFK Jr. is working with the HHS to release the gold standard evidence on vaccine injury, and once that comes out, the foundation has been laid for those rejecting vaccines to become the majority. This is extremely important, particularly since many are still advocating for vaccine mandates (e.g., I’ve received numerous concerned emails from readers that Hawaii’s left-wing physician governor will soon remove religious exemptions and hence mandate them,1,2,3 just like California’s Dr. Pan did). However, none of that can happen if the majority of America does not trust the vaccines and hence sees vaccines as a corrupt assault on their health and liberty.
Note: these trends are also demonstrated by a recent large JAMA study of 443,445 Americans, which found that in April 2020, 71.5% of them trusted doctors and hospitals, while in January 2024, only 40.1% did
Vaccine Propaganda
The actual evidence against vaccines is atrocious (e.g., independent studies all show they make you 3-10x more likely to develop a variety of chronic illnesses, and there is over a century of literature showing they cause profound neurological injuries). Because of this, the only viable way to maintain the vaccine market has been to prohibit all independent research on vaccine safety (which is why RFK’s government studies are so important) and gaslight the country.
At its core, propaganda exists to sell “unsellable” ideas to the public. To accomplish this, the sale must be emotional rather than logical, as indefensible ideas quickly dissipate when exposed to debate. As such, propaganda relies upon a variety of tactics which are emotional in nature but often masquerade as being scientific.
For example, much of propaganda revolves around using words that elicit emotional responses in people and having the media collectively reinforce that emotional reaction. As such, many debates, regardless of the arguments put forward often devolve into those emotionally charged slurs (e.g., “you’re a racist,” “you are a climate change denier,” “you don’t believe in science” “you’re an anti-vaxxer” “you are a peddler of dangerous conspiracies” “you’re a quack”). Because of this:
•Non-scientific positions are often erected by having a few false slogans to defend them which are shouted until they drown out any competing arguments (rather than the arguments being seriously considered).
•A lot of work goes into sculpting the most emotionally manipulative phrase (or imagery) which can support a desired narrative, at which point it is blasted throughout the entire mass media and then adopted by everyday people who come to believe the phrases were their own ideas.
More importantly, propaganda takes advantage of the fact people are naturally hesitant to stray from the crowd, and as such, if they hear the same message everywhere (particularly if their peers also adopt it), most will quickly adopt it too. Because of this, the mass media will collectively parrot the same messages, collectively denounce those who deviate from them, have an endless stream of “experts” on to defend the status quo, and most importantly, never allow the other side to be heard.
In turn, many of the major problems with medicine in our country ultimately from from a 1997 decision by the FDA to legalize television pharmaceutical advertisements, at which point, the pharmaceutical industry became the mass media’s largest advertiser. Soon after, that financial influence was leveraged to suppress media scrutiny, gradually eliminating news reports questioning the pharmaceutical industry—especially those about vaccines—making it nearly impossible to imagine critical news programs like those that once aired existing today.
Note: news anchors who witnessed this shift, like Sharyl Attkisson have attested to it.
Because of the blank check this monopoly on truth gave them, the vaccine industry became increasingly brazen in its actions (e.g., pushing more and more injurious vaccines onto the market, enacting more and more censorship, and then implementing more and more mandates). Fortunately, like many who suddenly rise to power, they overstepped and created a significant backlash, which has arguably left the industry in its worst position ever.
This is because, in addition to the mounting injuries (as the more vaccines children get, the more injuries they will have), an even larger backlash was occurring against the mass media in general, making it much harder for them to maintain control over unpopular narratives like vaccination.
Note: in recent decades, especially the last one, the media has gotten more and more aggressive in asserting its narrative (regardless of how nonsensical it is) while suppressing all dissenting ones. Since the internet has become integrated into the fabric of society, and well produced content (e.g., those debunking mass media lies the public is against) can rapidly go viral, the existing model no longer works. If anything, the more that it is doubled down on, the more people lose trust in it.
Contorting Medical Injuries
One of my morbid hobbies has been studying how pharmaceutical drugs injure and disable people and within this spectrum, I find the ones that create psychiatric issues alongside physical ones to be particularly cruel.
For example, SSRI antidepressants have many common side effects (e.g. sexual dysfunction, bipolar disorder, emotional numbness, terrible withdrawals and at times psychotic violence), many of which cause the individual to feel as though they are “losing their mind” and desperately want to stop the drugs. However, rather than recognize the drug is injuring them, the doctor will often tell the patient those side effects are due to the patient’s own mental illness rather than being a commonly recognized side effect of the drugs.
As such, the patient will be told to continue taking their drugs. Furthermore, since “mentally ill” patients are often deemed to lack the capacity to make their own judgment, whereas psychiatrists are seen as authority figures, I have seen more cases than I can count where everyone (e.g., the patient’s family and the courts [which frequently mandate treatment]) side with the psychiatrist rather than the patient, in turn all insisting those side effects are due to the patient’s mental illness and force the patient to take even more psychiatric drugs.
Note: this gets even more challenging for the patient when they begin to lose their grip on reality from the side effects of the drug and start questioning their own judgment, or if they should give up on themselves and just blindly trust the authority figures around them.
Some of the classic ways psychiatry gaslights patients include:
•Telling them that any symptom that emerges is due to the pre-existing mental illness.
•When a patient experiences adverse effects from a drug, the dosage is increased rather than acknowledging the side effects.
Note: this is a story commonly seen immediately preceding catastrophic school shootings, but unfortunately, since there is widespread denial in the psychiatric field that SSRIs can make patients turn psychotic, it is rarely recognized (hence leading to it happening over and over again).
•When a patient experiences withdrawal reactions (which is very common and one of the most insidious issues with the SSRIs), telling the patient that those side effects prove the patient “needed” the drug (as it was treating their mental illness) rather than it being recognized as a dangerous withdrawal effect.
•When a patient develops new psychiatric symptoms (e.g., mania) patients are told the drug did not “cause” the symptoms, but rather, that the drug “unmasked” a psychiatric disorder that had always been there (even though it would have never been “unmasked” if the patient had not used the drug in the first place). For example, bipolar disorder is a debilitating condition which around 25% of longterm SSRI users develop (hence leading to an epidemic of bipolar disorder ever since we started mass medicating with SSRIs), and since it is so common, the “unmasking” story has become the party line most psychiatrists use to rationalize the harm being caused to their patients.
Sadly, gaslighting is not unique to psychiatry. For example, throughout many of the clinical trials for the more toxic drugs on the market, trial participants developed severe side effects, but to ensure the pharmaceutical’s approval, those reactions were hidden both from the trial participants and the government by the clinical trial investigators. For example, I’ve detailed the appalling degree to which this was done in:
•The SSRI clinical trials.
•The HPV vaccine trials.
•The COVID vaccine trials.
Note: many were appalled by what whistleblowers shared happened in the COVID vaccine trials (e.g., everyone telling them a clear injury they had wasn’t “real”), but as I tried to illustrate in those articles, these are actually long standing problems in clinical trials (as they cost so much money to conduct, the pharmaceutical sponsors will do everything they can to “prove” the trial showed the drug was “safe and effective”).
Since doctors are trained to believe an injury is only “real” (rather than an anecdotal coincidence or simply imagined in the patient’s mind) if the injury is proven to exist within “unbiased” clinical trials, the gaslighting you see in the clinical trials sets of a chain of gaslighting as doctors around the world will believe what the clinical trials showed is true and hence dismiss the same injuries in their own patients which were covered up the clinical trials (and hence never made it to the final clinical trial report).
Note: since many different drugs cause neurological injuries (particularly in susceptible people) that are misdiagnosed as psychiatric injuries, this creates a huge problem, particularly since those patients are often fed into the psyche funnel, at which point they get put on even more neurologically destructive medications.
What is Gaslighting?
One of the classic ways an abuser controls their prey is to manipulate the environment so that the abused individual begins doubting their own observations, regardless of what is occurring in front of them.
In the 1944 movie Gaslight, this was accomplished by the villainous husband (played by Charles Boyer) adjusting the intake to gas-powered lights (causing them to flicker) and simultaneously denying that any change was occurring to his mentally abused wife (played by Ingrid Bergman). The term gaslighting originated from this classic movie.
In modern times, this is accomplished by having medical providers (and often mass media) all echo the same message that a patient’s injury has nothing to do with the pharmaceutical (or other medical procedure in question), and often blame it on the patient’s own psychiatric issues.
Before we go any further, I want to emphasize just how miserable this is to go through as an injured patient. Imagine what it would be like if (due to the medical injury) the world you had previously known collapsed around you and every single person you trusted (including your friends and family who defer to the judgment of “experts”) told you that it was all in your head and you just needed psychiatric help. It’s a perfect recipe for going insane.
For example, let’s consider the experiences of Maddie De Garay in the pivotal Pfizer trial that was used to argue for the safety of the COVID-19 vaccines in the adolescent population:
Although Maddie’s experience was atrocious, it was sadly not unique, and many others had similar experiences in the COVID-19 vaccine trials. Similarly, I have heard many similar stories from other people who were harmed by the medical system, as most pharmaceuticals have a degree of toxicity that will injure certain patients.
Since that toxicity has always been inherent to the practice of allopathic (Western) medicine, the profession has gradually come up with a playbook to prevent its inevitable medical injuries from sabotaging business. This has essentially been accomplished by doing the following:
•Telling patients the adverse events they experienced either are not occurring or are unrelated to the toxic pharmaceutical.
•Developing an elaborate scientific apparatus that provides evidence refuting the link between these injuries and pharmaceuticals on the market, while concurrently training the population to defer to the scientific consensus rather than trusting their own observations.
•Making competing forms of medicine that lack a similar degree of inherent toxicity illegal, therefore making the only choice within the existing medical marketplace be a toxic form of medicine (similarly consider how modern medicine is always considered to be the best form of medicine every other approach must find a way to measure up to).
This is also why we have the doctrine in medicine that every treatment has risks and the treatments are chosen because its benefits outweigh its risk (as opposed to just exploring systems of medicine without those risks).
All of this in turn results in the tragic phenomenon known as medical gaslighting, or as some like to put it “allopathic medicine gaslights you to death.”
Why Can’t Doctors Diagnose Medical Injuries?
I have found numerous documented examples of medical gaslighting stretching back to the late 1700s, and in each case, typically only a minority of the medical profession was willing to acknowledge that the injuries that were occurring could be linked to their pharmaceuticals.
At the same time, it’s rare for me to meet doctors I consider to be evil; on the contrary, most tend to be remarkably intelligent and well-intentioned individuals who genuinely want the best for their patients.
At this point, I believe medical gaslighting is a natural consequence of our training. Since the therapeutic toolbox of allopathic medicine is quite limited, most doctors cannot practice their craft without administering unsafe pharmaceuticals to their patients, and thus for the sake of their self-identity, they must fully believe in their pharmaceuticals (discussed further here).
Becoming a physician is an enormous personal investment, and it is extremely difficult for someone who has gone through that process to acknowledge that much of what they learned is highly questionable.
Similarly, no well-intentioned doctor wants to harm a patient, and since they often do, the reflexive psychological coping mechanism is to deny the possibility of each injury that occurs.
This first dawned on me when a doctor inserted a tirade against anti-vaxxers into his lecture and concluded his argument with “... and just think about it. Do you really think pediatricians would vaccinate their patients if they thought vaccines could harm them?”
Although widespread denial of the harms that Allopathy causes likely explains some of my profession’s predilection for gaslighting, I do not believe it is the primary issue. Instead, I believe it is a result of the training doctors receive making them unable to recognize medical injuries.
The Origins of Medical Blindness
Because the human body is immensely complex, humans in every era face significant difficulties in being present to everything that is occurring within a human being. Most medical systems address this challenge by creating diagnostic models which simplify the immense complexity present in each patient down to the key things that must be focused upon to positively affect patient wellbeing.
The downside to this approach is that there will always be things in each patient that lie outside the diagnostic model being used to evaluate them. When this happens, those things understandably will not be recognized unless the medical practitioner is a very talented and open-minded observer.
In the case of standard medicine, we are taught a diagnostic model that is excellent for identifying many things (particularly indications for prescribing pharmaceutical drugs). However, our model also fails to account for many other factors that are critical to health and wellness.
For example, much of medicine is taught by having a series of lists to memorize that are plugged into linear algorithms. Because this requires breaking many complex subjects into a binary “yes” or “no,” many important things that lie between these two polarities get lost in translation.
This is the easiest to illustrate with the nervous system (but the issue is by no means exclusive to it). When evaluating it, one of the things we are all taught to do is quickly check if the twelve cranial nerves are functioning normally (e.g., can you swallow, smile, or follow a finger with your eyes)?
Frequently, although the cranial nerves are “generally normal” they will have some difficulty firing (e.g., at some point in the motion arc as the eyes travel side to side, they will jump instead of moving smoothly). These “minor” deficits (which frequently follow microstrokes from vaccine injuries) often have a significant impact on a patient’s quality of life, but in most cases (except when evaluated by experienced neurologists or neurosurgeons), the function of those nerves will be noted as normal and ignored, and as such, doctors who can see the vast number of vaccine injuries around them are ostracized and dismissed by their colleagues.
Simplifying Illness
The cranial nerve example unfortunately is only one of many areas where a complex presentation of symptoms is simplified into a box that excludes an inconvenient diagnosis from ever being recognized. Another common way this boxing occurs is when an authoritative diagnosis is used to deny a complex phenomenon without actually stating what it is.
For example, many disorders in medicine are simply symptoms written in Latin. Dermatitis quite literally translates to “inflammation of the skin,” and in most cases is simply treated with a cream that suppresses that inflammation rather than an attempt to understand why the inflammation is there.
Conversely, in many other medical systems, inflammation of the skin is recognized as a crucial sign that something is amiss in the body, and the exact character and location of the inflammation are closely examined to identify and address the underlying cause of that inflammation.
Note: to some extent this is recognized in dermatology, but even there it occurs nowhere to the degree that it should.
In turn, I find that many common illnesses patients struggle with often have one or a few common causes; yet, in most cases, the underlying pathology is not examined or understood throughout their medical journey, even when top specialists in the field examine them. All of this, I would argue is a result of the medical system is not being structured to incentivize trying to understand the unique context of each person’s illness (rather doctors just get a few minutes to prescribe treatments targeting the patient’s symptoms in the hope one eventually works—which simultaneously often ignoring the harms of those pharmaceuticals).
Framing the Iatrogenic Debate
Iatrogenesis is the term for any type of illness or medical complication resulting from a bad reaction to medical care (e.g., a complication from a surgery or a pharmaceutical). A common pattern I’ve observed for decades is everyone denying a particular iatrogenic complication exists (e.g., “there is no evidence”), and then once overwhelming evidence exists that it does, it will be acknowledged.
Once this happens, the harm from the drug will be reframed so that only the accepted harm can be bad, and an underlying assumption is created that nothing else is a possible complication.
For example, fluoroquinolones (e.g., Cipro) are fairly toxic antibiotics that can severely harm people and are frequently given for many minor infections (e.g., urinary tract infections) where their corresponding toxicity is simply not justified for the potential benefit offered.
In medical school, everyone learns that a tendon rupture (something unique and hard to ignore) is a side effect of these drugs, and as a result, when doctors evaluate for harms, they will look for that but not be able to recognize most of the other well-documented complications from the fluoroquinolones.
Recently we saw this reframing occur with the J&J COVID-19 vaccine. At the start of Operation Warp Speed, I hypothesized that a major goal was to get mRNA technology onto the market since it held the promise of trillions of dollars in future revenue for the pharmaceutical industry (but since there were safety challenges with it, nothing short of an "emergency" would be able to break the barrier to human testing).
Because of this, I suspected that once vaccine safety concerns emerged, a non-mRNA COVID-19 vaccine would be thrown under the bus to make the mRNA technology look “safe.” This is what then happened with the J&J vaccine, when six cases of an extremely unusual blood clot were linked to that vaccine, causing the FDA and CDC to pause its administration for 11 days.
By doing so, it created the perception that the FDA was monitoring for vaccine side effects with a fine-tooth comb and was willing to pull the vaccine if it caused a rare side effect in a very small number of people.
Nothing could be further from the truth, as the mRNA vaccines have caused far more blood clots than the J&J vaccine. Similarly, investigation after investigation shows the FDA is ignoring the endless deluge of red flags from the COVID-19 vaccines.
Unfortunately, this ploy worked (temporarily), and for over a year in the odd instances where I hear a doctor willing to debate the safety of the vaccines, one of the most common arguments they would utilize is that if the FDA was willing to temporarily pause J&J after six blood clots, there is no possible way a larger unaddressed problem exists with the mRNA vaccines.
Likewise, the CDC has continually insisted there are no significant side effects from the COVID vaccine, but eventually was forced to concede that it could cause myocarditis. At that point, a pivot was made that said the myocarditis is very minor (which is not true), and that COVID-19 is more likely to give you myocarditis than the vaccine (so overall the vaccine actually prevents you from getting myocarditis)—which again is not true. As such, many attempts have been made to reframe the side effects of the vaccine to “the only issue with it is that it occasionally gives you brief myocarditis, but you do know it’s very minor and the actual myocarditis issue is from COVID-19.”
Psychiatric Complications and Iatrogenic Injuries
As the above points have shown, a variety of factors work against doctors being able to recognize the presence of medical injuries. The question then becomes, how will the injuries that inevitably occur be explained?
As you might imagine, the default strategy is to fold the injury into an amorphous diagnosis which can then take the blame for the medical injury and then put that label on everyone with the injury. Typically this is done with psychiatric diagnoses, but recently COVID-19 infections have also been appointed to that role (both of these diagnoses were used to gaslight patients in the clinical trials for those vaccines).
The earliest references to this gaslighting I have found were at the time of Freud, where his new model of psychoanalysis was used to explain the complex symptoms observed within patients that doctors otherwise had difficulty making sense of. However, as detailed in The Age of Autism: Mercury, Medicine, and a Man-Made Epidemic, an outside evaluation of Freud’s case studies suggests many of those patients’ problems actually arose from mercury poisoning.
Mercury, despite being extremely toxic, was used by the medical profession for centuries (and to some extent still is). Frequently, individuals with mercury poisoning would develop a wide array of complex diseases that included neurological and psychiatric complications (which, like many other conditions, were often attributed to “female hysteria”).
Freud’s message that these complications were the fault of the patient (e.g., as a result of unresolved sexual desires) rather than the physician, was an immensely appealing message to the medical profession, and as a result, became the party line.
Ever since this time there has been a systemic failure to recognize that neurologic damage can produce psychiatric symptoms. Instead, neurologic symptoms are viewed as a manifestation of a pre-existing psychological illness that must be treated with psychological counseling and psychiatric medications.
One of the best examples of this issue is “Functional Neurological Disorder” (FND) which recognizes that something is wrong with the brain, but since no explanation can be found, it is then assumed to have been due to pre-existing psychiatric conditions.
If you review the National Institute of Health’s description of FND, you will see that the above description is no exaggeration, and it is extremely sad to hear about the experiences vaccine-injured patients go through since FND is one of the most common diagnoses they receive.
When I look at FND cases (e.g., those characterized by seizures), the cause of the disorder can frequently be found, but since neurologists (including friends of mine) do not want to consider the actual cause, the tests needed to diagnose it are often not ordered or even known about by the doctors attending to the patient.
If you review Maddie’s story, you will note that this is also exactly what happened to her and her permanent paralysis from the vaccine was labeled as FND resulting from a psychiatric condition. Because of this gaslighting, she was not able to get appropriate care when her neurological reaction to the vaccine was occurring (that likely could have prevented permanent disability).
I believe this occurred because the chief investigator was fully aware that a severe neurologic reaction to a single participant would have made the vaccine too dangerous for children to take, so he decided to gaslight Maddie so her injury would not need to end up in the trial. Sadder still, Maddie’s experiences were not unique, and the testimonies we’ve received from trial participants clearly show there was systemic fraud in the COVID vaccine trials.
Another common symptom doctors place the blame for medical injuries on is “anxiety.” The two major problems with this process are:
Failing to recognize that having a life-changing injury will normally create distress, and similarly failing to recognize that being collectively gaslighted by medical providers is not good for anyone’s mental health. Worse still, pharmaceutical injuries frequently cause tissue damage that will trigger anxiety.
Note: furthermore much of the mass media controls us through creating anxiety about the future to sell the current product or narrative.
Sadly, very few doctors recognize that damage to the nervous system (which is a common toxicity of pharmaceuticals) can also create psychiatric disturbances. Instead, they can only recognize that psychiatric distress can often worsen neurologic symptoms, but do so without also realizing that it is much rarer for psychiatric distress to be the originating cause of a neurologic issue.
Similarly, many common psychiatric disorders have organic causes (e.g., chronic undiagnosed infections, traumatic brain injuries, or nutritional and metabolic deficiencies). However, in most cases, psychiatrists prescribe medications based on the symptoms a patient presents with (e.g., you are depressed so you need Prozac) rather than looking at the underlying cause.
I believe this is because doing the former pays well, but the latter typically does not and is not emphasized in a psychiatrist’s training.
In addition to neurological damage frequently creating psychiatric complications (e.g., vagal dysfunction creating anxiety), damage to other organ systems can as well (Chinese medicine does an excellent job of mapping these correlations out). One of the best examples I have seen with the COVID-19 vaccines relates to the heart and I have had variations of the following conversations multiple times since 2021:
Friend: I have been having severe anxiety attacks since I got the vaccine. My heart starts beating rapidly, and I start to have pain in my chest. I never had this problem before, but now everything makes me anxious and it’s so hard for me to be calm.
Me: You should get your heart looked at.
Friend: What do you mean? Everyone told me it was anxiety due to stress.
Me: Trust me, you need to get your heart looked at.
(Time passes)
Friend: How did you know I had myocarditis?
Damage to the heart (or the vagus nerve) will often create an irregular heart rate and chest pain, and these palpitations often provoke anxiety. Unfortunately, since these symptoms are also triggered by anxiety, when they are observed, doctors will often default to a diagnosis of anxiety and look no further.
Note: while I find this gaslighting is extremely common and problematic, it’s also important to acknowledge that there are psychiatric patients who are delusional (or dishonest) and see things that are not there. As such, challenging patients with very real medical injuries will often be placed into the same bucket as those patients, and even well-intentioned doctors who are aware of this will still sometimes encounter situations where they aren’t completely sure which scenario applies to their patient.
Medical Paternalism
There are essentially two models of medical practice that are followed:
The paternalistic model (where you are expected to unquestioningly trust and comply with everything the doctor tells you).
The collaborative model, where the physician is your partner in working towards health.
Although the paternalistic model was the standard for most of Western medicine’s history, in recent times, there has been a push for the collaborative model. Presently, many patients are seeking out collaborative physicians (especially since system doctors have to spend so much time going through checklists that there is little time for actual engagement with their patients), and the market is economically rewarding physicians who are making this change.
A key misconception much of the public holds about doctors is that we are infallible beings (which is a key justification for the paternalistic model). In reality, once you peer behind the lab coat, we struggle with many of the same issues you all do too. Being able to genuinely recognize this and respectfully treat the physician you see as a fellow human being is one of the most effective strategies for initiating a collaborative doctor-patient relationship.
Although doctors sometimes gaslight injured patients for self-serving reasons (e.g., to protect Pfizer’s vaccine in its clinical trials or under the severely misguided belief it will protect a doctor from a lawsuit), I believe the majority of cases occur because the doctors simply cannot see the injury occurred. As a result, these doctors believe they are doing the best for the patient when in reality they are just gaslighting them.
One of the largest issues in our modern era is how disconnected we have become from ourselves and others. Within the doctor-patient relationship, this disconnection makes it much less likely a physician will be able to recognize what is happening in a patient (e.g., a medical injury) or feel compelled to go to bat for them while every other healthcare provider is gaslighting them.
When people ask me for their best options to avoid being gaslighted, I thus suggest pursuing one of the following options:
1) See a physician whom you pay directly (rather than one who takes insurance). This business model matters because it forces the doctor to have a collaborative doctor-patient relationship and stay in business (no one will pay to see them if they just get gaslit). I am a big believer in the statement “you get what you pay for” and if you only see system doctors who base their practice around insurance payments, you often do not get a good outcome.
For example, shortly before I wrote an earlier draft of this article, I had a patient with what I felt was a relatively straightforward problem that had significantly impacted his life for 25 years. When I reviewed his history, he told me he had seen a dozen (insurance-taking) doctors, many of whom promised they could fix the problems with elaborate procedures from their specialty (all of which did nothing or made his issue worse).
What was striking about his story was that only one of them had ever even performed an extensive evaluation to try to figure out what was causing the problem.
2) However, while seeing a private-pay physician often is an excellent investment, many patients simply cannot afford to do so. In this case, the ideal scenario is to find an insurance-taking physician through word of mouth who has earned a reputation for forging collaborative doctor-patient relationships. Unfortunately, these recommendations are hard to come across, and typically these doctors will have full practices that are hard to get into.
3) The third (and often the only available option) is to take the initiative to forge a collaborative relationship with the doctor through having a respectful demeanor where you treat the doctor as a fellow human being rather than “the doctor.”
In general, this approach will be the most effective on doctors who recently completed their medical training (everyone becomes more rigid with age, plus early on, their practices are not yet full), and in medical settings where the doctors get longer per visit (you can’t really build a collaborative relationship in 10-15 minutes).
Regardless of the option you choose, it is also often important to provide the documentation to support the occurrence of your medical injury. This includes records establishing a timeline of the injury following the medical therapy and scientific literature substantiating the link between the two.
Physicians in turn (especially younger ones) will be the most receptive to considering this link if it is presented in a composed and thoughtful way rather than a confrontational manner, because like every other human they tend to become defensive. Given how upsetting the process of being gaslighted is, maintaining this demeanor can be extremely challenging.
Sadly though, it is necessary because doctors are trained to see pharmaceutical injuries as being psychological in nature, and a patient expressing their completely justifiable feelings about the situation will often feed into the doctor’s erroneous perceptions about the patient’s mental health.
Conclusion
Whenever governments are decaying, the audacity of their lies will increase more and more, which we likewise are seeing throughout the media (both with the vaccines and with our entire political process). While this approach can be quite effective (consider how many people still believe the narrative), at the same time, once it passes a certain point, everyone begins to wake up, especially if they have a framework to place those lies into context.
Put differently, many of the social changes we are now seeing are because people have become so fed up with the mass media’s over the top gaslighting about what we can see is happening in front of us with our own eyes. Since there are only two options for the media to address this (either more gaslighting or telling the truth), still, they aren’t willing to give up their power (or money) by telling the truth, they’ve boxed themselves into a downward spiral in public trust by continuing to double down on gaslighting.
Medical gaslighting is one of the things I despise most in medicine, and as such, it is one of my primary goals with this publication to bring attention to this concept. It has hence been incredibly encouraging to see that the fallout from COVID (and the profound gaslighting both patients and doctors received about their vaccine injuries) has made there be much more receptivity to the possibility of iatrogenic injuries, particularly from the COVID vaccine—what is happening now is completely different from anything I’ve seen in my lifetime. That is largely because each of you, and I am profoundly grateful that we may at last be moving to a point where medical gaslighting will end—particularly since the medical industrial complex is now losing so much money from lost trust, it is being economically forced to begin telling the truth to regain lost business.
To learn how other readers have benefitted from this publication and the community it has created, their feedback can be viewed here. Additionally, an index of all the articles published in the Forgotten Side of Medicine can be viewed here.



私は離婚してシングルマザーで、お金もあまりなかったので、緊急時以外は医者に行くことも、子供たちを連れて行くこともできませんでした。今にして思えば、それは幸運だったのかもしれません。ワクチンに関する医師のアドバイスに従っていたために子供たちに何かあったら、どれほどの恐怖と苦痛を味わうことになるか、想像もできません。かつてはワクチン接種が必要だったかもしれませんし、ヒポクラテスの誓いを掲げ、それに従って生きてきた医療従事者もいたでしょう。しかし、その後、私たちは全く異なる方向へ進んでしまいました。それは患者や子供たちにとって最善ではない方向です。私は二度とワクチン接種を受けることはありませんし、医療界にも強い疑念を抱いています。記事をありがとうございました。シェアしてくださる情報はすべて楽しく読ませていただいています。
あなたの視点とすべての記事に心から感謝していますが、今回の件は悲しみも伴います。このガスライティングを克服するための3つの選択肢は、ほとんど実行不可能です。「アフォーダブル」ケア法は、医療費をますます手頃なものにし、受診を困難にするだけでした。仲介業者である保険会社が治療の決定権を握り、費用を吊り上げています(価格交渉によって、保険会社は自動的に割引を行うため、以前と同じ利益を得るために医療提供者は価格を引き上げます)。コンシェルジュドクターの診察は、彼らが提供する治療以外は保険適用外であり、通常はネットワーク外の価格で行われます。しかし、年間費用は?あり得ません。人口の大部分は、それを支払う余裕がありません。「ドクターショッピング」――現実的に考えてみてください。誰かが、このような患者と向き合う意思のある医師のデータベースを作成する必要があります。単に医師名簿から医師を選ぶだけでは、現実的な選択肢ではありません。
25歳から30年間ベータ遮断薬を服用していたことが、私の神経系に長期的な(そしておそらく修復不可能ではない)ダメージを与えたことを認め、その治療法を見つけてくれる医療専門家を、ほぼ10年間探し求めてきました。55歳の時に心臓専門医から服用をやめるように言われ、徐々に減らしていくことなく服用を中止した後、症状が急激に悪化しました。助けを求めたとき、かかりつけ医の答えは?「その薬が原因ではないはずです。せいぜい2週間で体から抜けます」でした。その言葉は私も分かっていますが、30年間服用していた薬が、私に何かを与え、それは消えることはありません。ようやく少し改善が見られるようになりましたが、それは2016年に起こりました。彼女の解決策は?ベンゾジアゼピン系薬剤でしたが、それがさらに症状を悪化させたのです!
最近、内分泌科医に相談したいと思いました。おそらく数十年前から高インスリン血症、あるいは糖尿病予備群だったのだと思います。それが動脈硬化を引き起こし、CABG×4手術を受けることになりました。64年間、誰か私のA1C値や空腹時インスリン値を検査した人はいたでしょうか?一度もありませんでした。しかし、LDL-C値については、本当にしつこく尋ねられました。内分泌科医は2型糖尿病の流行でかつてないほど忙しくなっています。6ヶ月後にようやく診察を受けることができました。彼の最初の質問は「なぜここに来たのかわかりません」でした。それから彼は、保険会社に検査、基本的な検査の正当性を証明するために、診断書を作成しなければなりませんでした。幸いにも彼は私の話を聞いてくれて、高血圧を診断書として提示してくれました。
対症療法の世界への信頼度はほぼゼロです。緊急時以外は、自分で血液検査をして自分で診断します。どうもありがとうございます。私自身ほど自分の健康を気にかけている人はいません。忍耐強く、自らを癒せ。